Foreword:
In the modern world there is no place for such problems as the inferiority of a person who has lost a limb. Scientists and experts in the field of medicine and engineering have formed a community of people involved in prosthetics. The aim of such a community is to help patients with amputation of limbs to feel adequate again. Experts create companies for the mass production of prosthetic products, and scientists around the world help to improve this product by bringing the mechanism closer to a realistic limb [1,2].
According to statistics, among 100,000 children aged 0-17 y.o., in 2005 15% of children with amputation of a limb were accounted for, in 2010 – 10.2%, 2013 – 9.7%, 2014 – 9.9%, 2015 – 9.5% [3]. Children are our future, and these statistics indicate a further annual loss of an average of 10% due to the inferiority of the new generation in the intellectual and industrial development of the world. The task of today’s generation is to help this layer of the population to feel united with society.
In this article we consider one of the urgent problems in the field of prosthetics and try to put forward a number of hypotheses that should lead to an answer to the problems raised.
Formulation of the problem:
An important point in creating a prosthesis is to create a high-quality control system, because this place is the point of interaction between the living and the nonliving. Scientists from different countries have devoted multiple articles and practical works in the field of creating a perfect prosthesis management system [4,8,10] to this issue. Among the many solutions to this problem, one can see how researchers are looking for their answer in various fields of science from mechanics to human neurophysiology. But you can observe the main 2 rows of scientists: the first, who are looking for an answer to improve the existing standard control system built on electromyography; and the second, who go towards the unknown and try to find the answer in building a new prosthesis control system based on electroencephalography. Let’s look at each method in more detail. We’ll clarify right away that in this article and our subsequent scientific works we will consider a non-invasive method of signal registration using sensors from a patient, therefore, the considered scientific works are also based on the same method.
Speaking about electromyography as the basis of current control systems, it is necessary to understand that this system as a whole is formed on the registered signals from the patient’s muscles, where, with a reduction in the fiber group, changes in current from 0.6 to 3.0 mA and voltage from 0.2 to 1 are observed , 7 uV. The control system data consists of sensors registering signals from the patient, a processing module with a set of software filters for signal cleaning, and a decision module based on reference images of ideal signals [5,6,7].
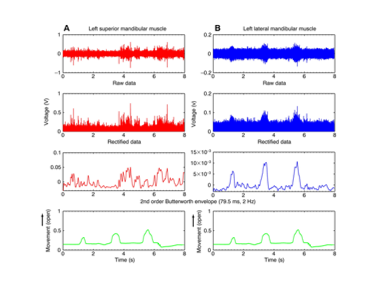
Figure 1. Graphs of the signals of contraction of 2 muscle groups taken using EMG.
In Figure 1, you can observe the process of filtering two signals from different muscle groups and comparing them with the ideal control signal. First, the signal from the sensor is obtained, then the signal goes through 2 stages of filtering, where it is eventually converted into a monochrome signal without noise. It was these actions that were carried out with the red and blue signals shown in Figure 1. Next, the signals are checked against the graph of the ideal control signal, green. The coincidence in the voltage spikes of the blue graph with the green signal shown below tells us about the recognition of movement and the definition of one of the commands. However, in this paper there are a number of subtleties. To begin with, the number of recognition of various types of grip according to recent calculations is 13-15 grips [9]. This amount is enough to implement most of the human activity, however, the overall quality of recognition of these types of grip in such systems is currently 78%. The duration of such signals lasts about 20-25 ms, and the process of fixing, transmitting, filtering, recognizing, determining and realizing the movement of the prosthesis itself increases the time of the whole process, creating a delay and turning it into a painful 7-9 sec response. Many patients are willing to put up with such delays. But we are talking about the usefulness of a person, which means that while driving or any other emergency, the patient is obliged to take action in a split second. Time and quality of recognition are the enemy of such control systems.
If we consider a typical EEG-based prosthesis control system, then it consists of a registration module receiving EEG signals from the patient; processing module with built-in filters to clean the signal from noise, from artifacts that store patterns of images of ideal signals; a rating generating comparison module used to identify the most likely movements or to decide on the truth of the movement performed by the patient. The signals caused by various stimuli emanate from various areas of the brain and vary greatly in frequency range and amplitude [11,12].
To determine the nuances in the difference in frequency ranges and amplitudes, we need to consider the process of signal registration in more detail.
The location of the electrodes in such processes is usually carried out according to the scheme 10-20 recommended by the International Federation of electroencephalography and clinical neurophysiology. These numbers 10 and 20 indicate that the distance between the electrodes should be 10% – 20% of the length of the line connecting two such reference points as nasion (nose bridge) and anion (occipital protuberance) [13].

Figure 2. Arrangement of EEG electrodes.
Figure 2a and 2b shows the standard arrangement of 21 electrodes, and figure 2c shows the arrangement of 75 electrodes. This circuit is an extended electrode circuit that provides high spatial resolution, which improves the accuracy of recognition of control signals for various parts of the body. It is important to understand that to determine the type of grip and movement of the hand, we need to record the readings of only a specific part of the brain. In Figure 3, we can observe that the region of interest to us is located in the left and right hemispheres in the middle plane of the precentral gyrus of the brain and the cortical part of the analyzer of the general sensitivity of a person.

Figure 3. Areas of the brain responsible for various parts of the body.
The most significant brain activity corresponds to a range from 0.5 to 40 Hz, inclusive. There are five main rhythms distinguished in the EEG signal: delta, theta, alpha, beta and gamma. The peak voltage values of such EEG signals are about 100 μV when measured on the scalp and about 1–2 mV when measured directly on the surface of the brain [14,15].
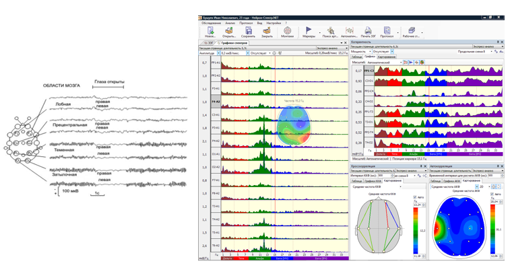
Figure 4. Electroencephalogram using a concentrated analysis of the cerebral cortex in areas responsible for the human motor apparatus
So, for example, in Figure 4, using the extended electrode circuit, but at the same time, collecting the signal only from the zones of the hemispheres in the middle plane of the precentral gyrus of the brain and the cortical part of the analyzer of the general sensitivity of a person, we can fix that the speed of the signal at different rhythms goes from 5 up to 300 ms. Such a big difference allows us to make consistent verification of the signal and improve the quality of determining the type of hand grip we need. However, in such systems there is a clear problem, if you increase the recognition rate of the image, bringing it closer to the flow rate in the EMG, there is a decline in the quality of recognition of the grip. As a result, such systems have a high speed of detecting the image of the hand movement itself, but suffer from the accuracy of recognizing the type of movement.
In the course of a general analysis of both systems, we can conclude that not one of the systems can give the full probability of recognizing the type of grip. The electromyography method currently has a high quality signal recognition, but does not have small time indicators. The electroencephalogram method, on the contrary, has a low recognition rate, however, the quality of determining the type of grip is only 43%.
Solution Concept / Hypothesis:
Against the background of such obvious drawbacks and advantages of the two systems, a hypothesis is created about the creation of a mixed prosthesis control system based on two previously presented methods. The hypothesis is based on the fact that, using a high signal speed due to the electroencephalogram method, we can build a prediction system for prosthesis control processes, and the electromyography method can not be overloaded with the signal verification time interval and can only be used to improve the quality of grip recognition. However, the question immediately arises of how to build the structure of interconnections, what lies in the core of decision-making, which of the systems has a high level of prioritization, and on what to base the motion prediction system. Figure 6 shows the concept of a mixed control system, where the nuclear process of the forecasting and decision-making system is taken as the basis.
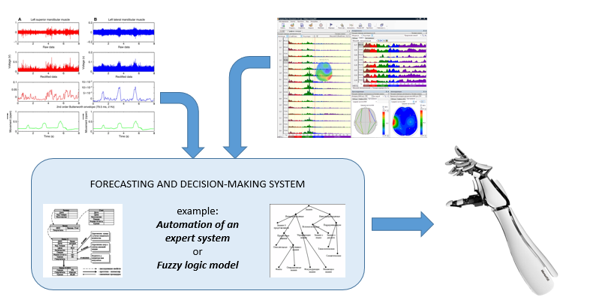
Figure 6. The concept of a mixed prosthesis management system based on a forecasting and decision making system.
The methods of artificial intelligence are considered as the construction of core processes, but it is not yet clear how this or that method will behave, we will focus on two methods: expert systems and fuzzy logic. These methods have the following characteristics: lack of hasty conclusions; issuing an optimal solution; unlimited knowledge base sizes; simplicity in execution.
Conclusion:
Our team of researchers has already begun to develop this system, but it is worth noting that during the course of work we encountered some difficulties in synchronizing processes. The first important point in the problem that arises is the lack of consideration of the reaction time of a person. This parameter is the time it takes for a person from the moment the incident was recorded to the moment of the response, and it is equal, on average, from 100 to 180 ms. So, from the moment of recognition of the electroencephalogram system to the moment of recognition of the electromyography system, a delay appears that increases the duration of the system’s response.
Another problem is the difficulty in filtering the signals both at the stage of the EMG signal system and at the stage of the EEG signal system. Everything has an effect: the level of tissue damage, the thickness of the fat and skin, the abundance of the hair.
Of course, the developed system is also required in statistical analysis on a large number of respondents. A similar step in this research is essential to achieve stable results of use regardless of the patient.
In conclusion, it is worth noting that this hybrid prosthetic control system is difficult to implement, and often for professional people it seems unattainable. However, if we collect all the works of scientists and empirically try to compile the material into a single system, this will allow us to bring the prosthesis management system to a new stage.
Reference:
- Metzger, A., Dromerick, A., Holley, R., Lum, P.: Characterization of compensatory trunk movements during prosthetic upper limb reaching tasks. Arch. Phys. Med. Rehabil. 93(11), 2029–2034 (2012)
- McFarland, L., Hubbard, S., Heinemann, A., Jones, M., Esquenazi, A.: Unilateral upper-limb loss: satisfaction and prosthetic device use in veterans and service members from Vietnam and OIF/OEF conflicts. J. Rehabil. Res. Dev. 47, 299–316 (2010)
- FEDERAL STATE STATISTICS SERVICE (Rosstat) HEALTH CARE IN RUSSIA 2017, Statistical Bulletin, Moscow 2017, p. 70
- S. POO, K. Sundaraj “Design and Development of a Low Cost EMG Signal Acquisitions Systems Using Surface EMG Electrode” Asia Pacific Conference on Circuits and System (APCCAS), 2010, p. 24-27
- Liu, Y.w., Feng, F., and Gao, Y.f. (2014). Hit prosthetic hand based on tendon-driven mechanism. Journal of Central South University, 21, 1778{1791.
- Dhillon, GS and Horch, KW (2005) Neural sensory feedback and control of a prosthetic arm, IEEE Transactions on Neural Systems and Rehabilitation Engineering 13, 468-472.
- Carrozza, MC Persichetti, A Laschi, C Vecchi, F Vacalebri, P Tamburrelli, V Lazzarini, R and Dario, P (2005) A novel wearable foot interface for controlling robotic hands, 2005 IEEE/RSJ International Conference on Intelligent
- Robots and Systems (IROS 2005), 2010 – 2015. DARPA http://www.darpa.mil/dso/solicitations/ prosthesisPIP.htm [accessed 3/4/20]
- Clark A (2013) Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behav Brain Sci 36:181–253
- Feinberg TE, Mallatt J (2016) The nature of primary consciousness. A new synthesis. Conscious Cogn 43:113–127
- Sherman SM (2016) Thalamus plays a central role in ongoing cortical functioning. Nat Neurosci 19:533–541
- Tononi G, Boly M, Gosseries O, Laureys S (2016a) The neurology of consciousness: an overview. In: Laureys S, Gosseries O, Tononi G (eds) The neurology of consciousness, 2nd edn. Academic Press, San Diego, pp 407–461
- Tononi G, Boly M, Massimini M, Koch C (2016b) Integrated information theory: from consciousness to its physical substrate. Nat Rev Neurosci 17:450–46
- H. van Hateren (2019) A theory of consciousness: computation, algorithm, and neurobiological realization, Biological Cybernetics (2019) 113:357–372
- Nan Bu, Masaru Okamoto, Toshio Tsuji, (2009) A hybrid motion classification approach for EMG – based Human –robot interfaces using Bayesian and neural natworks, IEEE Transaction on robotics, vol. 25, no. 3
